Remote Therapeutic Monitoring Billing & Program Management
Why RTM Fits Interventional Pain
The Pain Epidemic
Pain is common, high-impact, and expensive.
U.S. Adults
24.3%
Report suffering from chronic pain in 2023.
High-Impact
8.5%
Pain limiting life activities on a daily basis.
RTM bridges episodic pain care with continuous patient outcomes, transforming "between-visit work" into billable treatment.
Clinical Impact
Early flare detection, faster plan adjustments, and standardized outcomes based on real-world data.
Operational Efficiency
Reduce inbound calls via digital check-ins; efficient triage saves MD/APP time for high-value visits.
Financial Health
Generates recurring revenue streams, minimizes denials through documentation, and optimizes reimbursement.
RTM Billing: The 4 Codes That Matter
Understanding these four CPT codes is essential for RTM billing.
98975
Setup + Education Frequency: Once per RTM episode Requirements: Patient onboarding (device/app) and PRO education.
98977
Device Supply (MSK) Frequency: 16–30 qualifying days per 30-day period Requirements: Collect PRO data & adherence; document qualifying days.
98980
Treatment Mgmt Frequency: First 20 minutes per 30-day period Requirements: Data review, treatment decision, and one interactive communication.
98981
Additional Time Frequency: Each additional 20 minutes (same month) Requirements: For extended treatment management. Must be with 98980.
Compliance Note: 98977 requires documented qualifying days. 98980/98981 need documented time and interactive patient communication.
The RTM Process: What Actually Happens
A reproducible workflow for scalable, defensible RTM, defining ownership and documentation.
01
Identify Candidates
Select post-procedure or chronic pain patients suitable for monitoring.
02
Enroll + Consent
Obtain consent, complete setup (98975). Document education & activation.
03
Monitor Daily
Collect PRO/adherence data. Verify 16–30 qualifying days (98977). Store raw data.
04
Manage + Intervene
Review data, clinical decisions. Document time & interaction (98980/81).
05
Report + Bill
Generate monthly summaries. QA check by RCM team. Submit claims.
Staff Role Allocation
MA/Coordinator
Enrollment, reminders, device tracking, data collection.
RN/Coach
Triage, patient education, escalating clinical exceptions.
MD/APP
Clinical judgment, treatment decisions, complex outreach, attestations.
RCM Team
Claim QA, denial management, billing optimization.
Compliance Checklist: What Auditors Look For
Audit success hinges on thorough documentation. Undocumented clinical work is unbillable.
- Device Days (98977)
- 16–30 qualifying days per 30-day period.
- Document start/stop dates and records.
- Retain raw PRO/adherence data.
- Time + Interaction
- Document actual time in 20-minute increments.
- Record one interactive communication monthly.
- Link actions to patient plan adjustments.
- Documentation Gaps
- Missing device-day logs.
- Time documentation without specific activities.
- Undocumented interactive communication.
- Clinical decisions not tied to monitored data.
- Missing provider signature/attestation.
Addressing these gaps eliminates 80% of potential denials.
- Medical Necessity
- Document diagnosis and rationale for monitoring.
- Show how data impacts decisions/interventions.
- Specify monitored data and clinical relevance.
- Pre-Bill QA Process
- A monthly "pre-bill QA" checklist reduces denials and accelerates cash collection. Weekly denial reviews and monthly underpayment audits increase revenue.
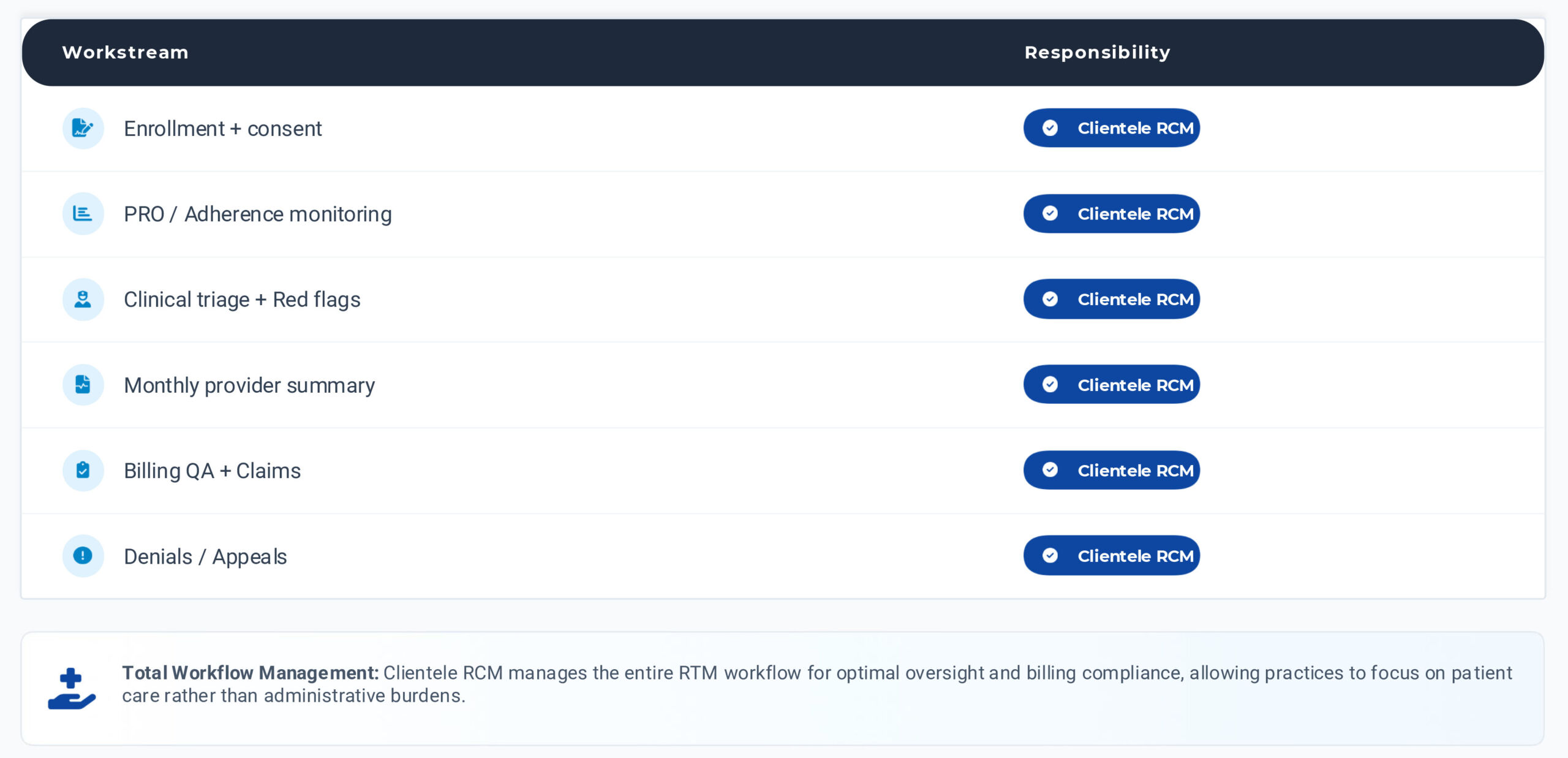
Operating Model for Pain Practices
Delegate routine tasks to free MD/APP for high-value decisions, ensuring efficient workflow.
Reimbursement Benchmark: Medicare Fee Schedule
Illustrative 200-patient RTM model using 2024B national Medicare Physician Fee Schedule payments.
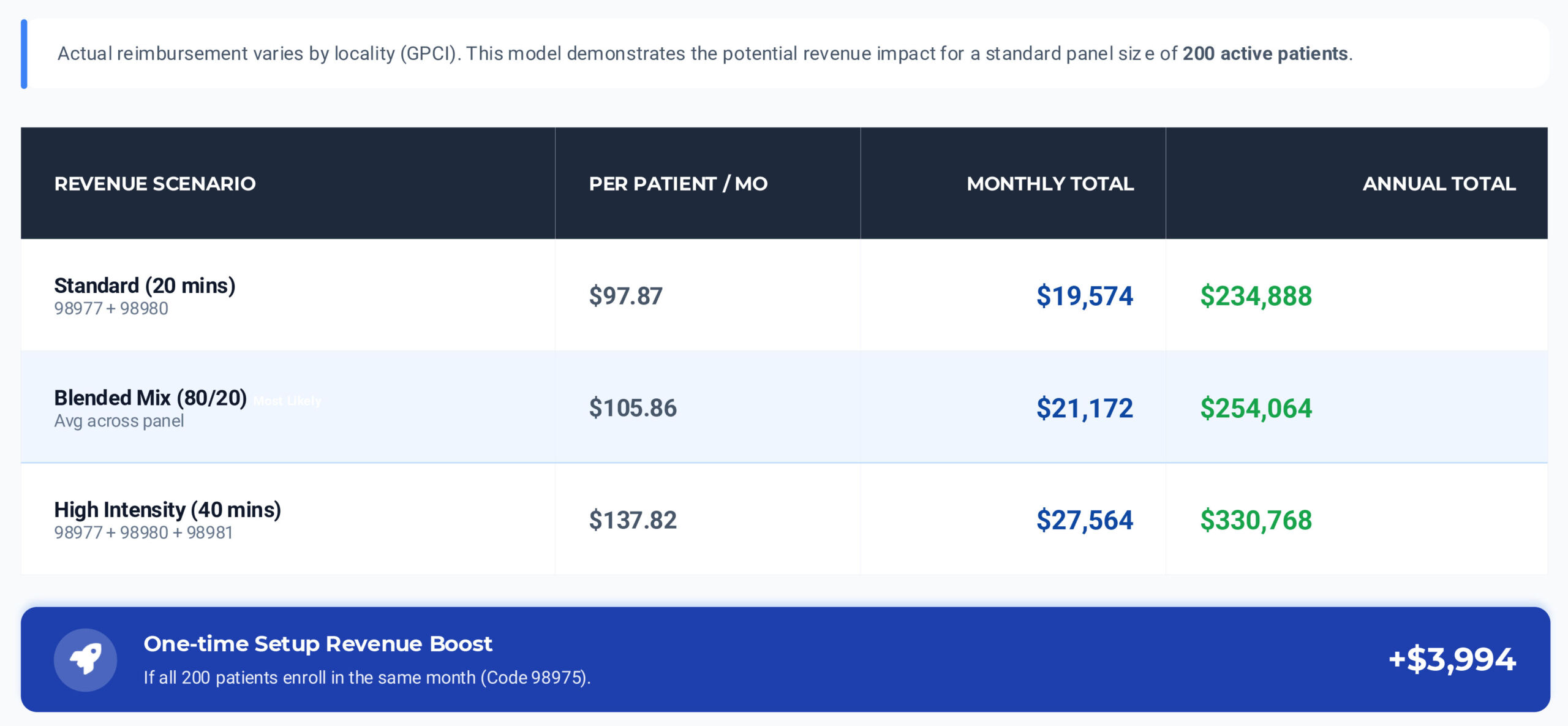
*Projections assume patients meet monthly device-day (16–30 days) and time documentation requirements. Blended scenario assumes 80% standard / 20% high intensity mix.
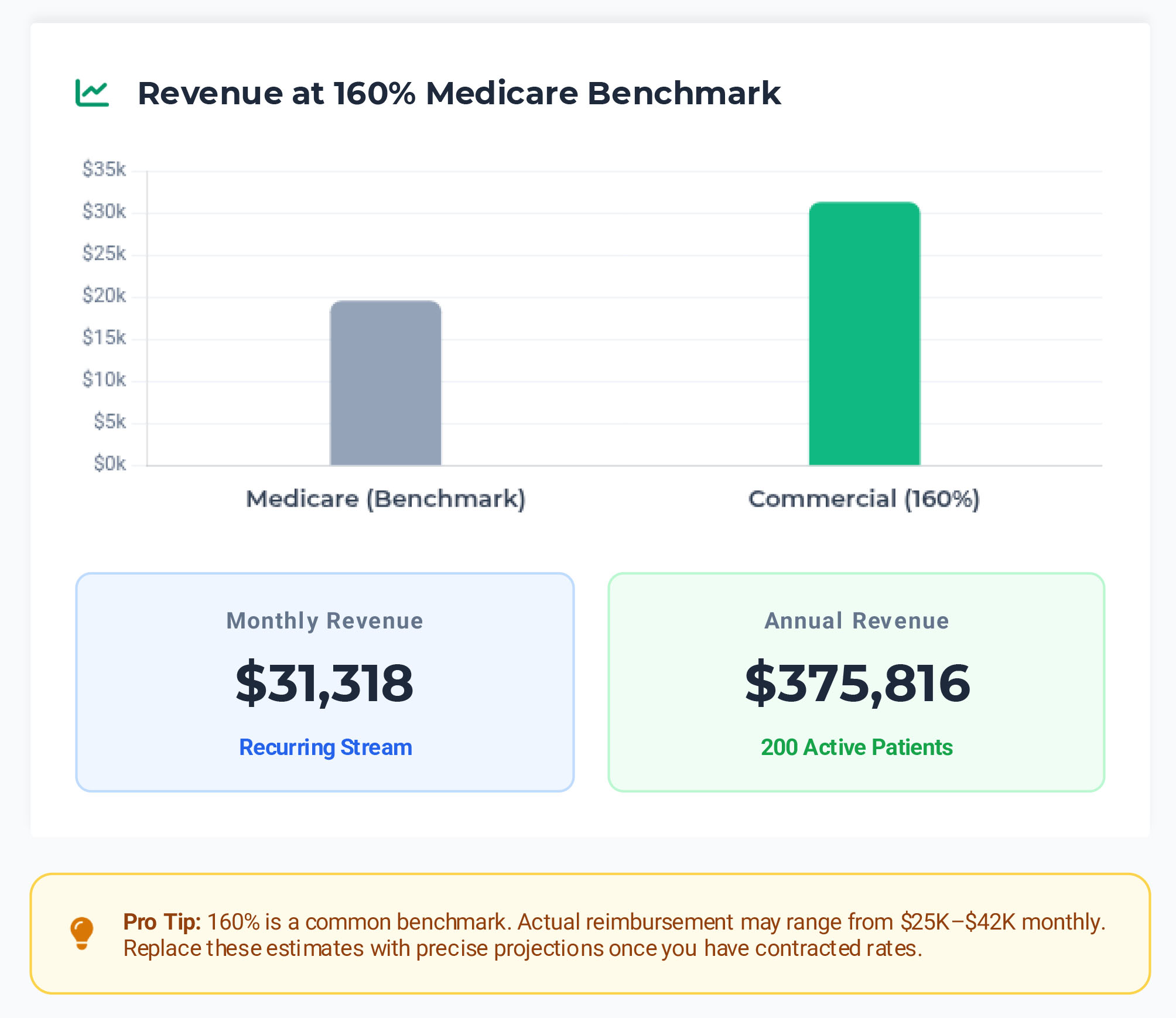
Commercial Reimbursement: Fast Modeling
Model commercial reimbursement as a percentage of Medicare rates, then refine with actual fee schedule data.
- Commercial Payers: Key Differences
Allowed Amounts
Typically 140–220% of Medicare rates depending on payer contracts and locality.
Coverage Policies
May require specific medical necessity documentation or prior authorization unlike standard Medicare.
Denial Patterns
Often due to missing qualifying days or insufficient documentation of clinical decision making.
30-60-90 Day Launch Plan
Launch with a single cohort to prove workflow, then scale to 200 active patients.
Days 0-30
Design + Pilot
Patient Selection
Identify single cohort (e.g., post-RFA) for pilot.
Clinical Workflow
Finalize PRO schedule, escalation protocols, summary formats.
RCM Setup
Confirm eligibility checks, fee schedules, and claim edits.
Initial Enrollment
Onboard 25–50 patients to test flow.
Days 31-60
Operationalize
Workflow Cadence
Establish daily/weekly queue reviews for MA/RN/Providers.
Documentation
Standardize provider summaries with attestations.
Quality Control
Run pre-bill QA and submit first batch of claims.
Panel Growth
Scale program to 75–120 patients.
Days 61-90
Scale + Optimize
Denial Analysis
Review outcomes, identify patterns, refine payer playbooks.
Revenue Recovery
Detect underpayments, short-pays, or bundling errors.
Engagement Optimization
Refine comms to improve qualifying-day hit rate.
Full Scale
Reach target of 150–200 active patients.
Track Success
Key Performance Indicators
Enrollment Rate
Target > 80%
Qualifying Days
Achievement ≥ 70%
Denial Rate
< 5% by Month 3
Satisfaction
High Provider Score
Cash Flow
Speed to Collect
What You Get When RTM Is Run Correctly
Properly executed RTM delivers enhanced patient care, improved clinical outcomes, and predictable recurring revenue.
Medicare Benchmark
Standard Rates
$19,574
Per Month
160% Commercial Model
Common Commercial Rate
$31,318
Per Month
200% Commercial Model
Upper Commercial Rate
$39,148
Per Month
- Pilot Success Metrics
- ≥70% qualifying day achievement
- Denial rate <5%
- Queue-to-action SLA <48 hours
- High provider satisfaction score
- Next Step
- Pick a patient cohart, confirm payer coverage, and launch a 50-patient pilot within 30 days.
- Optional: Share California commercial contracts for tailored projections.
Why Choose Clientele RCM?
Clientele RCM ensures a seamless, compliant, and profitable Remote Therapeutic Monitoring program.
RTM Expertise & Compliance
Deep understanding of RTM regulations and billing, ensuring audit-proof documentation and claims integrity.
Operational Efficiency
We handle the entire RTM workflow, from enrollment to data monitoring, freeing up your clinical staff.
Maximized Revenue
Dedicated Support
Proactive guidance and responsive assistance from a dedicated RCM team invested in your practice’s success.
Focus on Patient Care
Delegate administrative burdens, allowing your providers to prioritize direct patient care and clinical outcomes.